Table of Contents
1. Aims and Scope
Respiratory Endoscopy, an official open-access journal of the Japan Society for Respiratory Endoscopy (JSRE), is a peer-reviewed, multidisciplinary journal directed to respiratory endoscopy physicians and scientists. The journal provides comprehensive and up-to-date peer-reviewed reference information on the techniques, procedures and recommendations in the field of respiratory endoscopy including bronchoscopy, thoracoscopy and closely related subjects. The journal publishes original articles, review articles, case reports, technical reports, images, brief communications, letters to the editor and guidelines/statements. The Journal is published three times each year (March, July and November).
The journal requires that all manuscripts be prepared in accordance with the “Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly work in Medical Journals.” as published by the International Committee of Medical Journal Editors (ICMJE).
2. Article Types
Respiratory Endoscopy publishes a variety of different article types. Once you have determined the correct Article Type, it is imperative that you read the Manuscript Preparation guidelines before you submit your manuscript:
3. Manuscript Preparation
Information provided here on manuscript preparation and formatting is based, in part, on the “Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals” as published by the ICMJE. For any information that is not mentioned in this guideline, authors should refer to the ICMJE Recommendations.
Manuscripts that do not follow the instructions below WILL BE RETURNED to the corresponding author for technical revision before undergoing peer review.
3.1 General Formatting
All articles should be written in English using size 12, "Times New Roman" font type and correctly formatted according to the guidelines outlined below. All text should be double-spaced. Line numbers and page numbers on each page are required to make it easier for reviewers to provide comments.
The organization of the manuscript should be in the following order:
3.1.1 Title Page
The title page should be prepared separately from the main document and must include the following information:
3.1.2 Main Document
Abstract and Key Words
Manuscript should include an abstract that includes the following headings, depending on the article type:
The Abstract, regardless of the Article Type, should contain 2-5 key words. The abstract must be precise, clear and fully comprehensible on its own. The Abstract of clinical trials must include the registration number and name of the registration database. See further details on clinical trials section below.
Main Text
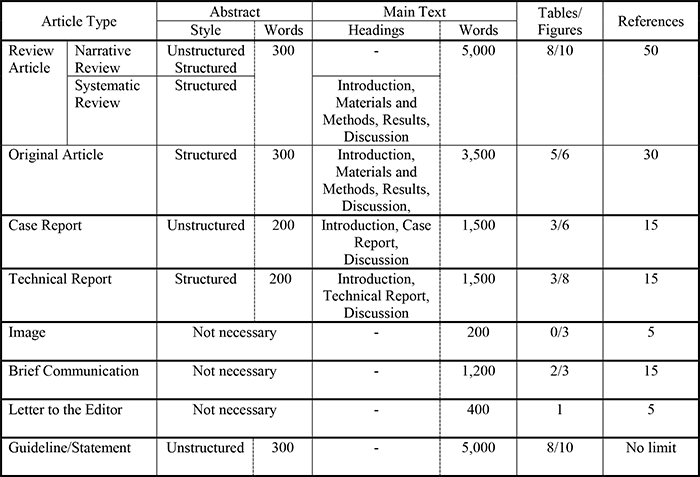
The main text should be prepared in MS Word (.doc or .docx). For each Article Type, authors must organize and order their content using the following formats:
Review Article:
Headings:
-Narrative Review: Not required
-Systematic Review: Introduction, Materials and Methods, Results, Discussion
Word Limit: 5,000 words
Number of Tables: No more than 8
Number of Figures: No more than 10
Number of References: No more than 50
Original Article:
Headings: Introduction, Materials and Methods, Results, Discussion,
Word Limit: 3,500 words
Number of Tables: No more than 5
Number of Figures: No more than 6
Number of References: No more than 30
Case Report:
Headings: Introduction, Case Report, Discussion
Word Limit: 1,500 words
Number of Tables: No more than 3
Number of Figures: No more than 6
Number of References: No more than 15
Technical Report:
Headings: Introduction, Technical Report, Discussion
Word Limit: 1,500 words
Number of Tables: No more than 3
Number of Figures: No more than 8
Number of References: No more than 15
Image:
Number of Authors: No more than 5
Word Limit: 200 words
Number of Figures: No more than 3
Number of References: No more than 5
Figure legend should not be contained.
Brief Communication:
Word Limit: 1,200 words
Number of Tables: No more than 2
Number of Figures: No more than 3
Number of References: No more than 15
Letter to the Editor:
Number of Authors: No more than 5
Word Limit: 400 words
Number of Tables and Figures: No more than 1
Number of References: No more than 5
Guideline/Statement
Word Limit: 5,000 words
Number of Tables: No more than 8
Number of Figures: No more than 10
Number of References: No limit
Subheadings are numbered in the order of 1. → 1) → (1).
3.2 References
The authors are responsible for the accuracy of their references. The References section should follow immediately after the conclusion of the main text under the heading "References". Authors must cite references in the text in the order of their appearance, showing the citations as superscripts (for example, show in superscript1). Three or more consecutive citations should be indicated as a range using a hyphen, e.g. "3-5". If there are more than three authors, name only the first three authors and then use “et al.”
Examples:
Journal article
1.Guiot BH, Khoo LT, Fessler RG. A minimally invasive technique for decompression of the lumber spine. Spine. 2002;27(4):432-8.
Journal article in a language other than English
2.Paroussis D, Papaoutsopoulou C. [Porcelain laminate veneers (HI-ERAM)]. Odontostomatol Proodos. 1990;44(6):423-6. Greek.
Homepage
3.Complementary/Integrative Medicine [Internet]. Houston: University of Texas, M. D. Anderson Cancer Center; c2007 [cited 2007 Feb 21]. Available from: http://www.mdanderson.org/departments/CIMER/.
Entire book
4.Jenkins PF. Making sense of the chest x-ray: a hands-on guide. New York: Oxford University Press; 2005. 194 p.
Book chapter
5.Riffenburgh RH. Statistics in medicine. 2nd ed. Amsterdam (Netherlands): Elsevier Academic Press; 2006. Chapter 24, Regression and correlation methods; p. 447-86.
Preprints
6.Bar DZ, Atkatsh K, Tavarez U, Erdos MR, Gruenbaum Y, Collins FS. Biotinylation by antibody recognition- A novel method for proximity labeling. BioRxiv 069187 [Preprint]. 2016 [cited 2017 Jan 12]. Available from: https://doi.org/10.1101/069187
Journal names should be abbreviated in the standard form as they appear in the NLM Catalog. If the journals are not included in the NLM Catalog, use the ISSN List of Title Word for standard abbreviations of journal names. If you are uncertain, please use the full journal name.
For reference styles pertaining to other media formats or further details, please refer to Citing Medicine, which is published by the National Library of Medicine (US).
Including AI-generated material as the primary source in the reference is not allowed.
3.3 Units of Measurement
Measurements of length, height, weight, and volume should be reported in metric units (meter, kilogram, or liter) or their decimal multiples. Temperatures should be in degrees Celsius. Blood pressures should be in millimeters of mercury. All measurements should follow the International System of Units (SI). Except for ℃ and %, one space must be inserted between each number and unit.
Use a capital letter "L" for liter in the units of measurements in the Text, Figures, and Tables (e.g., g/dL, mg/dL, IU/L, and mEq/L).
3.4 Abbreviations
Do not include the abbreviations in the title except for gene names or in commonly used abbreviations. Define abbreviations at their first appearance in the text and in each Table and Figure and use the abbreviations consistently thereafter.
3.5 Names of Drugs, Devices, and Other Products
Do not use the specific brand names of drugs, devices, and other products and services, unless it is essential to the discussion. Otherwise, please use descriptive name.
3.6 Figures and Tables
Figures and Tables should be numbered with Arabic numerals (e.g. Figure 1, Figure 2, Table 1, Table 2), and must be cited in the text in bold in the order they are cited
If any copyrighted or previously published material, edited or otherwise, are used in the manuscript, it is the author’s responsibility to obtain the permission from the copyright owner(s) prior to making a submission. Also, the authors must cite the source and indicate the permission to use such materials in the corresponding Figure or Table caption, as required by the copyright owner(s).
3.6.1 Figures
All illustrations (line drawings and photographs) are classified as figures. Figures should be submitted in the following digital format: JPEG (.jpg), or Tagged Image Format (.tiff).
Figures supplied within the main manuscript Word document or previously copy-and-pasted in PowerPoint are not acceptable. This is due to their low resolution. They will not re-produce in print or online clearly.
Scanned images of line art will not be accepted – please supply in the original file format.
Tone art, or photographic images should be produced at the minimum resolution of 300 dpi. All microscopic images (including light microscopy and scanning electron microscopy) must include information on magnification used at the time of image capture (e.g. "Original magnification ×400" or "Magnification ×10,000"). A clearly labeled scale bar (e.g. "Bar = 50 μm") should also be included in the image whenever possible.
All figure titles and legends should not be embedded in the submitted image – please supply this information separately (such as figure legends in the main manuscript file).
All extraneous use of color must be removed from Figures and Tables. Color should only be used for didactic purposes. All line art backgrounds must not contain any color.
3.6.2 Figure Legends
Legends must be prepared for all Figures presented in the manuscript and should be understandable without reference to the text. Authors must list Figure Legends on a separate page after the References section.
Figure legend is not required for the article type “Image”.
3.6.3 Tables and Footnotes
Tables are required to be in MS Word (.doc/.docx) or PowerPoint (.ppt/.pptx). Do not use MS Excel or comparable spreadsheet software. The Table captions should be understandable without reference to the text. Column headings should be kept as brief as possible and indicate units. Footnotes should be labeled a), b), c), etc. and typed on the same page as the table they refer to. Tables must be configured in a horizontal layout only.
3.6.4 Supplementary Materials
Respiratory Endoscopy accepts supplementary materials that may contain additional figures, tables or supporting movies. The authors should submit the supplementary materials as “Supplemental File” during the manuscript submission process via ScholarOne Manuscripts submission system. All video files should be submitted in MPEG-4 (.mpg) format. Refer to the supplementary materials starting with S1, S2 (e.g. Fig. S1, Table S1, Movie S1) in the manuscript's main text. Supplementary materials are published exactly as they are received and not edited by the journal. All supplementary materials will be published alongside the article on the journal website.
3.6.5 Graphical Abstract
Submission of a Graphical Abstract is optional. Authors who wish to have a Graphical Abstract published must upload it at the time of submission.
The Graphical Abstract should consist of a single image that visually represents the primary findings of an article, or alternatively, one of the figures or tables included in the manuscript may be used.
The file must be in .jpg format. When uploading, select the file designation "Graphical Abstract" in the submission system.
Note: Even if you use a figure or table from the manuscript, it must be uploaded separately from the manuscript's figures/tables with the file designation "Graphical Abstract."
4. Clinical Trials
In accordance with ICMJE’s policy on trial registration, all clinical trials must be registered with a public trials registry before the time of first patient enrollment. ICMJE defines clinical trials as any research project that prospectively assigns people or a group of people to an intervention, with or without concurrent comparison or control groups, to study the cause-and-effect relationship between a health-related intervention and a health outcome. Health-related interventions include, but are not limited to, those used to modify a biomedical or health-related outcome; examples include drugs, surgical procedures, devices, behavioral treatments, educational programs, dietary interventions, quality improvement interventions, and process-of-care changes.
Respiratory Endoscopy requires all clinical trials to be registered with databases that are accessible to the public at no charge, open to all prospective registrants, managed by a not-for-profit organization, have a mechanism to ensure the validity of the registration data, and are electronically searchable.
Submitted manuscripts must include the unique registration number in the abstract as evidence of registration. The name of the registration database must also be provided. For details regarding the required minimal registration data set, please go to the ICMJE site at http://www.icmje.org/recommendations/browse/publishing-and-editorial-issues/clinical-trial-registration.html
The journal accepts registration from the following list of registries as well as others listed at ICMJE site:
In reporting randomized clinical trials, authors must comply with published CONSORT guidelines (http://www.consort-statement.org/). The recommended checklist must be completed and provided to the journal at the time of manuscript submission. The recommended trial flow diagram should be presented as“Supplementary File”.
5. Reporting Guidelines
Various reporting guidelines have been developed for different study designs. Authors are encouraged to follow published standard reporting guidelines for the study discipline.
Please access https://www.equator-network.org to find the guideline that is appropriate for your study.
It is extremely important that when you complete any Reporting Guideline checklist that you consider amending your manuscript to ensure your article addresses all relevant reporting criteria issues delineated in the appropriate reporting checklist. The purpose of a reporting guideline is to guide you in improving the reporting standard of your manuscript. The objective is not to solely complete the reporting checklist, but to use the checklist itself in the writing of your manuscript. Taking the time to ensure your manuscript meets these basic reporting needs will greatly improve your manuscript, while also potentially enhancing its chances for eventual publication.
6. Data Sharing
Respiratory Endoscopy encourages the authors of manuscript which includes clinical trials to share their de-identified research data including, but not limited to raw data, processed data, software, algorithms, protocols, methods, materials, study protocol, statistical analysis plan, informed consent form, clinical study report, analytic code.
As required by ICMJE, all manuscripts that report the results of clinical trial must include a data sharing statement with a link to the trial registration. The statement should include the following information:
The statement is published alongside their paper.
7. Online Manuscript Submission
Manuscripts may only be submitted electronically via the journal’s ScholarOne system: https://mc.manuscriptcentral.com/respend
Simply log on to ScholarOne Manuscripts and follow the onscreen instructions for all submissions. You will need to register before your first submission to Respiratory Endoscopy. If you have any technical problems or questions related to the electronic submission process or uploading your files, please contact our Support Desk. For other inquiries, please contact the Editorial Office:
ScholarOne Manuscripts Support Desk (Japan)
Phone: +81-3-3910-4517, E-mail: s1-support@kyorin.co.jp
All files must be submitted in the following order: 1) Title Page, 2) Main Document, 3) Tables, and Figures (≥300 dpi). The total size of the uploaded files should be within 100 MB. Upon submission, the manuscript will be automatically checked for plagiarism, and can be sent back to the corresponding author if the plagiarism rate is 30% or higher.
Notification of manuscript submission will be sent by e-mail to all authors listed in the manuscript.
8. Peer Review Process
Articles submitted to Respiratory Endoscopy are subject to a single-anonymized peer review process. This means the identities of the peer reviewers remain anonymous but the authors’ identities are known to the reviewers. Peer review is a critically important process of evaluation for any manuscript submitted to Respiratory Endoscopy. Every article dispatched for full peer review will receive a comprehensive, fair, and unbiased critical assessment.
All submitted manuscripts will be reviewed, initially, by the editors of Respiratory Endoscopy to evaluate eligibility for publication. The editors will assess the importance and originality of the research, suitability and interest to the readership of the journal, and the quality of the manuscript. Any manuscripts that satisfy our screening criteria will generally be sent to two experts in the field of the study for peer review. The editors of Respiratory Endoscopy will review the peer review comments and make all decisions on the manuscript publication, which include acceptance, major or minor revisions, and rejection.
Respiratory Endoscopy adheres to Committee on Publication Ethics’ Ethical Guidelines for Peer Reviewers. Reviewers are not allowed to contact the authors directly before, during, or after the peer review process to discuss any information that is presented in the manuscript. Reviewers must keep the manuscripts and information obtained strictly confidential and must not publicly discuss or disclose the contents and any other information contained within the manuscript to a third party. The guidelines for the reviewers are available here.
The decision letters along with the comments by the editors and reviewers will be sent to the corresponding author via e-mail.
8.1 Revised Manuscript
It is expected that any manuscripts receiving a revision decision will be fully amended according to the comments of both the reviewers and the editors. Authors must also include a detailed point-by-point response letter. Authors should submit the revised manuscript within 3 months from the date of prior decision. Revisions must be approved by all authors prior to submission of the revised manuscript.
8.2 Editors and Journal Staff as Authors
Manuscripts submitted by editors, Editorial Board members, or journal staff will follow the same process as outlined above. However, they are excluded from any editorial decision process of their own manuscript and have neither access to that manuscript nor any information about the review process other than what is provided in the editor’s decision letter. Additionally, ScholarOne, the journal’s online submission and peer review system is designed to anonymize a person in other roles (editor/reviewer) from any paper he/she has authored. The manuscript submitted by editors, Editorial Board, and journal staff of Respiratory Endoscopy should include a statement that declares their personal conflict of interest with the journal.
9. Editorial Policy and Publication Ethics
9.1 Overview
Respiratory Endoscopy observes the highest standards in journal publication. The journal supports and adheres to the guidelines and best practices including Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals by the International Committee of Medical Journals Editors (ICMJE) and the Principles of Transparency and Best Practice in Scholarly Publishing (a joint statement by the Committee on Publication Ethics (COPE), the Directory of Open Access Journals (DOAJ), the World Association for Medical Editors (WAME) and the Open Access Scholarly Publishers Association (OASPA); (https://doaj.org/apply/transparency/)).
9.2 Authorship/Contributorship
All authors listed in the manuscript must meet the following four contribution criteria as defined by the ICMJE in their Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals.
1) Substantial contributions to the conception or design of the research or the acquisition and analysis of data; and
2) Drafting the work or reviewing it critically for important intellectual content; and
3) Final approval of the version to be published; and
4) Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Contributors who do not meet all four criteria above should not be listed as authors. Guest or honorary authorship is strictly prohibited.
In consonance with the COPE’s position statement and WAME’s recommendations, Respiratory Endoscopy does not allow Artificial Intelligence (AI) tools such as ChatGPT or Large Language Models (LLM) to be listed as authors as those tools cannot meet the ICMJE’s criteria for authorship listed above.
The corresponding author must ensure that a manuscript is read and approved by ALL authors prior to submission.
Those who do not qualify for authorship may be acknowledged individually or together as a group under a single heading within the “Acknowledgements” on the title page. Examples of activities that do not qualify a contributor for authorship are: acquisition of funding; general supervision of a research group; general administrative support and writing assistance; technical editing; language editing, and proofreading.
Authors should discuss, determine and (if they exist) settle any disagreements about the order of authorship before submitting their manuscript. Final author order must be established by the end of the revision phase of the peer review process. Any authorship changes such as order, addition, and deletion of authors between the initial manuscript submission and the final decision should be discussed and approved by all authors. Any request for such changes must be explained in the Change of Authorship Request Form, which must be signed by all authors.
Adding, deleting, or changing the author names and their order is not permitted after the acceptance of the manuscript for publication.
Use of Artificial Intelligence (AI)-Assisted Tools/Technologies
In consonance with the COPE’s position statement, WAME’s recommendations, and ICMJE’s Recommendation, Respiratory Endoscopy does not allow artificial intelligence (AI)-assisted tools/technologies such as Large Language Models (LLMs), chatbots, or image creators to be listed as author or co-author. As described in the ICMJE, those tools cannot be responsible for the accuracy, integrity, and originality of the work, thus they do not meet the ICMJE’s criteria for authorship listed above. The authors (humans) are fully responsible for any materials of the submitted work, including the use of AI-assisted tools or technologies. AI should not be cited as authors. Authors (humans) are also responsible for plagiarism including the in text and AI-produced images. Authors must disclose, upon submission and in the Materials and Methods (or similar section), any use of AI-assisted tools or technologies in the writing of a manuscript, production of images or graphical elements of the paper, or in the collection and analysis of data.
9.3 Exclusive Submission
Articles that have been previously published or are being considered for publication in another journal in any language will not be accepted. Submission of a manuscript implies that: the work described has not been previously published; it is not under consideration for publication elsewhere; its publication has been approved by all co-authors. The editors make all decisions on the acceptance of the peer-reviewed manuscripts.
9.4 Confidentiality
All manuscript details, author information, reviewer identities, comments to the editors and the authors, and the content of the decision letter are considered privileged information and will never be disclosed to third parties.
9.5 Redundant or Duplicate Publication
Articles that are being considered for publication in another journal including advanced publications such as “in-press” or “E-pub ahead of print” articles in any language might be regarded as redundant or duplicate publication.
The author should notify the editor formally about all submission and the previous reports that could be regarded as redundant or duplicate publication of the same or similar work. Any such material must be referred to and referenced in the new work. Copies of such work should be included with the submission. Abstracts or posters presented at scientific meetings are not considered previously published work. For studies that have been presented at a scientific meeting, “Acknowledgements” should include a sentence, such as "A part of this study has been presented at the XXth Annual Meeting of XXXXX (Month, Year, City)".
Editorial actions should be expected if redundant or duplicate publication is attempted or occurs without such notification. Editorial actions may include: immediate rejection of the submitted manuscript; retraction of published work; published notice of violation, and revocation of publishing privileges.
For acceptable secondary publication Respiratory Endoscopy accepts secondary publications of only those that meet the criteria and conditions described in the ICMJE Recommendations.
9.6 Conflicts of Interest and Sources of Funding
According to the ICMJE Recommendations, a conflict of interest (COI) exists “when professional judgment concerning a primary interest (such as patients' welfare or the validity of research) may be influenced by a secondary interest (such as financial gain).”
All authors are required to disclose any financial relations, activities, relationships and affiliations that exist, or have existed, in the 36 months (3 years) prior to submission with any commercial organizations, groups, institutions, or any other entities that has any interest in the subject matter, materials, or process(es) discussed in the manuscript. This includes, but is not limited to:
Any possible COI related to the study presented in the manuscript must be disclosed on the title page under the heading “Conflicts of Interest” using the following examples for each author:
“A (author name) received honoraria from Z (entity name); B holds an advisory role in Y; C is an employee of Company X.”
If the manuscript is accepted for publication, the disclosures will be published as they appear in this section. If there are no COIs, the authors should state “The authors declare that there are no conflicts of interest” on the title page.
All sources of funding from entities such as government or non-profit organizations, which are relevant to the study, should be acknowledged on the title page under the heading “Sources of Funding.”
9.7 Research Ethics
A) Clinical research included in articles that report on human subjects or materials of human origin, must comply with the provisions of the Declaration of Helsinki. In addition, the “Materials and Methods” section must include a statement that the research was approved by the IRB of the authors’ affiliated institutions and the approval code issued by the IRB and the name of the institution, which granted the approval. Those researchers who do not have access to an ethics review committees should follow the principles outlined in the Declaration of Helsinki.
B) Articles reporting on data from animal testing must indicate in the “Materials and Methods” section the approval of the testing design by the affiliated institution’s Animal Care and Use Committee.
C) Authors of articles reporting on new DNA sequences must furnish that data to the GenBank and include the accession number for it in the article.
D) For any studies involving human subjects it should be stated clearly in the text that written consent has been obtained from all patients (or parent or legal guardian) to publish the information, including their photographs.
E) Any data or information such as patient names, initials, hospital patient identification codes (patient IDs), specific dates, or any other information which may identify patients must not be presented anywhere in the manuscript, including the Figures and Tables unless the information is essential for scientific purposes and the patient (or parent or legal guardian). All pictures should focus on the affected areas only.
9.8 Misconduct and Breach of Publication Ethics
10. Proofing and Revision after Acceptance
After the acceptance of a manuscript for publication, a certificate of publication will be issued. Also, accepted manuscripts for publication will be proofed by the Editorial Office. Portions of the manuscript requiring corrections will be noted with comments indicating that the material must be rewritten. Galley proofs will be available to the authors for corrections of minor errors such as spelling errors and omitted characters or letters. Any other corrections and revisions after the acceptance of a manuscript are not permitted unless requested by the Editorial Board of Respiratory Endoscopy. Authors are expected to perform the proofing, as instructed by the Editorial Office. Upon completion of the proofing, authors should immediately email the revised proof to the Editorial Office.
After publication, further changes, or corrections, can only be made in the form of an Erratum which will be hyperlinked to the original article.
11. Copyright
Copyright to articles and their contents published in Respiratory Endoscopy belong to the Japan Society for Respiratory Endoscopy. However, Respiratory Endoscopy applies the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/) to all works published by the journal. Anyone may download, reuse, copy, reprint, distribute, or modify articles published in the journal, if they cite the original authors and source. No permission is required from the publisher. The license can be found on the last page of the published PDF of the article.
12. Charges
If the first author of the manuscript is a NON-MEMBER of the Japan Society for Respiratory Endoscopy:
Review Article: 100,000 JPY
Original Article: 100,000 JPY
Case Report: 100,000 JPY
Technical Report: 100,000 JPY
Image: 100,000 JPY
Brief Communication: 100,000 JPY
Letters to the Editor: Free of Charge
Guideline/Statement: 100,000 JPY
If the first author of the manuscript is a MEMBER of the Japan Society for Respiratory Endoscopy:
Review Article: 50,000 JPY
Original Article: 50,000 JPY
Case Report: 50,000 JPY
Technical Report: 50,000 JPY
Image: 50,000 JPY
Brief Communication: 50,000 JPY
Letters to the Editor: Free of Charge
Guideline/Statement: 50,000 JPY
Once your manuscript is accepted for publication in Respiratory Endoscopy, you will receive a confirmation e-mail which contains the instructions for making a payment. The APC is non-refundable.
13. Advertisement Policy
The Journal accepts advertising and sponsorship of the Journal, according to the following principles:
For inquiries:
Respiratory Endoscopy Editorial Office
E-mail: respend@kyorinmail.jp



